




The Democratic Republic of Congo reported a record single-day rise in Ebola on June 13, with the health ministry confirming 72 new cases as the outbreak reached its one-month mark.
The ministry said 29 deaths were recorded on the same day, bringing the outbreak total to 782 confirmed cases and 181 deaths since it was first detected a month earlier.
Most infections remain concentrated in the northeastern provinces of Ituri, North Kivu and South Kivu, and authorities said the number of affected health zones has climbed to 31; Nia-Nia in Ituri and Mabalako in North Kivu reported cases for the first time.
Uganda has recorded spillover from the DRC, with 19 confirmed cases and two deaths that the World Health Organization said are largely linked to cross-border transmission from the DRC.
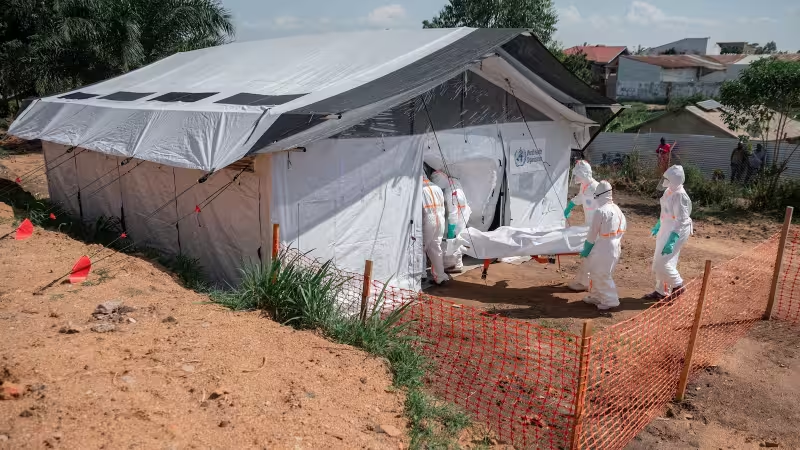
The immediate consequence of June 13’s surge is operational strain: health teams must track more exposures across a wider geography while managing care and safe burials. U.S.-funded partners reported screening more than 6,300 people in Ituri, supporting 100 health facilities and carrying out 200 safe burials, and the U.S. State Department said it plans to provide $50 million to CEPI while committing more than $270 million directly to the Ebola response.



Response teams face a critical gap in contact tracing. Health officials acknowledged they have followed up on only 56.5% of identified contacts — well short of the World Health Organization’s 90%–95% target — a shortfall officials attribute to community hesitance and shortages of medicines and infection-control supplies.
The shortfall matters because unchecked contacts are the most direct path for the virus to spread. United Nations agencies warned last week that children in eastern DRC were at heightened risk, and UNICEF said tracking the number of affected children could be unreliable because surveillance systems are not capturing cases consistently.
Public health experts have pressed that household transmission could drive the next phase of the outbreak. Dr. Douglas Noble warned that, as the response evolves, household spread may increase and that already vulnerable children could be disproportionately affected as families and community services come under added pressure.
That warning tracks with the outbreak’s footprint: more health zones, fresh case clusters in Nia-Nia and Mabalako, and cross-border chains into Uganda. The Bundibugyo strain is driving the current epidemic and, with only slightly more than half of contacts being followed, surveillance is not yet at the standard experts say is required to interrupt transmission.
The central unanswered question is whether contact follow-up can be scaled to the 90%–95% range the WHO recommends. With 782 cases documented and the recent spike of 72 new confirmed infections, the response will need rapid improvements in tracing, community engagement and supplies to avoid further geographic spread and greater impact on children and other vulnerable groups.






