




The European Centre for Disease Prevention and Control has published a clear set of risk categories and follow-up rules for travellers returning from areas affected by the 2026 Ebola virus outbreak caused by Bundibugyo virus.
At the center of the guidance are three practical answers travellers and public health teams need now: who counts as having no exposure, who counts as a protected occupational exposure, and who counts as a higher‑risk or unprotected exposure — and each category carries a distinct 21‑day monitoring expectation.
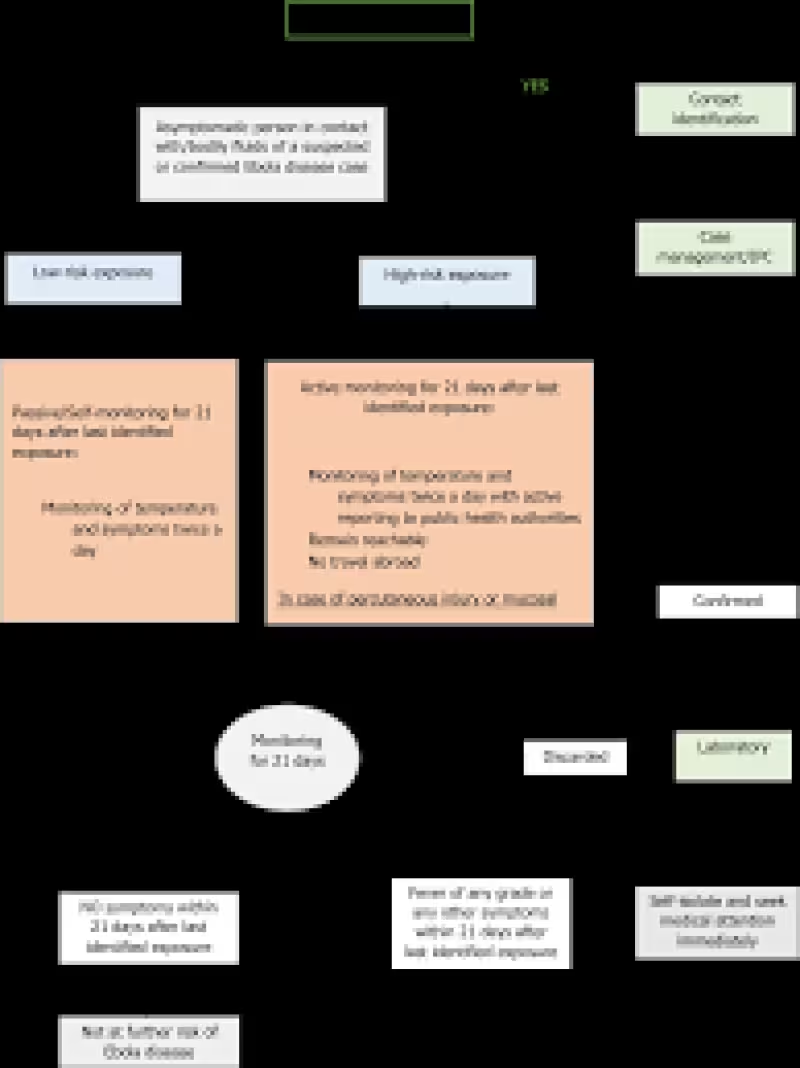
People who had no exposure — meaning they had no contact with symptomatic cases or persons under investigation — are not placed under active surveillance. They should, however, receive clear, accurate, up‑to‑date information about Ebola disease, how it spreads, which symptoms to watch for, and targeted behavioural instructions on what to do if symptoms develop after arrival.
Health workers or laboratory staff who had properly protected contact with a suspected or confirmed Ebola case, with bodily fluids, fomites or virus samples are treated as having a protected occupational exposure. Those people must self‑monitor for 21 days after their last exposure, checking temperature and symptoms twice a day and following the guidance given to them on what to do if signs appear.
Higher‑risk contacts are those who had close face‑to‑face contact within less than 1 meter, any direct unprotected or improperly protected contact with a person who has suspected or confirmed Ebola disease, unprotected sexual contact with someone who has Ebola disease or a survivor without confirmed negative semen RT‑PCR tests, participation in burial rites with direct contact of remains or fluids without PPE, or percutaneous injury or mucosal exposure to suspect laboratory specimens. People in these categories should undergo active monitoring for 21 days following the last exposure, checking temperature and symptoms twice a day and actively reporting to public health authorities or responding to regular contact from those authorities.
The guidance draws a line around properly used personal protective equipment: contact while wearing appropriate PPE is not considered a significant exposure. That distinction matters for whether someone is moved into active surveillance. But ECDC emphasizes a practical caveat: doffing PPE is a vulnerable moment. If doffing is not done under a controlled protocol, observed by a trained person, it can create an elevated risk of self‑contamination and change a protected exposure into a higher‑risk one.
Public health authorities retain discretion to take further measures depending on circumstances. For example, where sexual exposure is a concern, the guidance identifies the role of RT‑PCR testing of semen and points to protocols that use two negative tests at least one week apart as part of declaring a negative status.
The operational consequences are straightforward. Returning travellers who fall into the protected occupational category must be given the tools to self‑monitor and a clear line to report symptoms; higher‑risk contacts will be enrolled in active follow‑up for 21 days and must check twice daily and report to authorities. Travellers with no exposure should still be briefed so they can recognise symptoms and act quickly if illness begins.
What the guidance does not say is how many travellers will be under each category or how many people are currently being monitored; that figure was not provided. That omission leaves an important gap for planners: resource needs for contact tracing, isolation capacity and clinical follow‑up depend on the size of the exposed population, and those numbers shape how aggressively authorities will act at ports, clinics and workplaces.
The pragmatic bottom line is this: if you returned from an area affected by the 2026 Bundibugyo virus outbreak, your status depends on what kind of contact you had. No exposure — information and watchful waiting. Protected occupational exposure — self‑monitor twice daily for 21 days. Unprotected or close contact, burial or percutaneous/mucosal exposure — active monitoring and reporting for 21 days. And whether you wore PPE or not, every step of putting it on and taking it off must follow controlled procedures; doffing done badly can erase the protection it provided.






